Sponsorship: A New Imperative For Leaders

by Dorothy Sisneros and Kevin Monaco
Impact of the sponsorship
Dorothy Sisneros
Have you ever been a sponsor or mentor? Or have you been sponsored or mentored? Chances are that at this point in your leadership journey, you have experienced one or all of the development opportunities offered by your organization or have hired external coaches to assist with your goals. In this blog, Kevin and I will explore the nuances and role of mentorship and sponsorship support and how you can become a protégé or sponsor a protégé regardless of your current role in an organization. The path to advancement for women and minorities usually includes being sponsored. Therefore, organizations should consider adding sponsorship to their talent management and succession planning programs.
I have had many amazing sponsors and the odd part is that until the last six months, I didn’t have an official term for what I had benefited from along my journey. I had mentors and coaches help me hone my skills and figure out what I wanted to do and where I wanted to be professionally. In reading several articles, I became aware of sponsorship and realized that my life has been shaped by the fact that several of my sponsors considered me a protégé and that my talents and abilities had been shared with an audience who were receptive to the amplification, boosting, connecting, and defending (Chow, 2021) from my sponsors.
Teachers can be our first sponsors as they open doors, write letters of recommendation, and help guide us into careers they hope will be a match for us. My first sponsor was my high school English teacher and basketball coach. Mr. Richard A Martinez (RA) was an exceptional teacher and incredible coach. He decided that college was in my future and that attending on a basketball scholarship was possible. He connected with the new Women’s Athletic Director at the University of Arizona and my role as a protégé began. He told Dr. Mary Roby about my athletic abilities, my academic strength and shared his endorsement of me as a person.
RA was my first sponsor – he found an audience (Dr. Roby) and connected her to me by telling stories and creating a positive impression. He amplified my abilities by sharing my accomplishments, boosted my potential and readiness for the college basketball experience, and defended me by ensuring her that a small-town “star” would be fine at a large university. Thanks to RA, I attended the University of Arizona on a basketball scholarship and I didn’t let him down. RA was my brand manager and publicist in the days before YouTube, Instagram or TikTok. I share this story as an example of the importance of a sponsor in our lives. I have had several other amazing sponsors and I’m grateful for each of them—I have been a willing protégé.
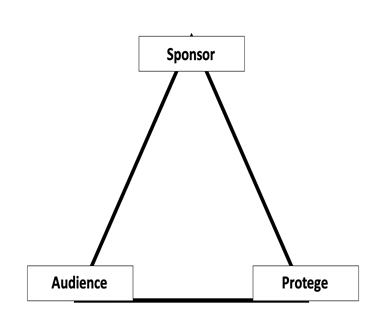
So, what is the difference between a sponsor and mentor? A mentor is someone who can provide immediate support in the form of guidance, advice and is usually someone who has had similar experiences in the job or position within an organization. The relationship is between the mentor and the mentee. In sponsorship, there is a 3-way relationship between the sponsor, the protege and the audience (Diagram 1). Chow (2021) stresses that sponsorship opportunities for minorities and women need to be intentional. For me, a Latinx woman from a small community of fewer than 100 residents, my path to success was linked to one sponsor who intentionally helped me by using his social capital and persistence to open the door for me and then walking with me into a new world. I still am connected to RA Martinez – we text every day and I can always count on a positive message from him to start my day.
I have taken on the sponsorship role with zest and am intentionally sponsoring several individuals who I admire and respect. I am using my social capital, my connections, and my influence to open doors and walk them through to meet others who can benefit from their talents and potential. I’ve been called a connector and I am proud of that title.
As I reflect, I am grateful to my sponsors – Rosalie Vigil, Richard (RA) Martinez, Dr. Mary Roby, Dr. Amy Steinbinder, Linn Billingsley, Mary Briden, Dr. Marie Pepicello, Dr. Rufus Glasper, Mary Lou Bessette, Sandy Shroyer, April Myers, Dustin Fennell, Dr. Wendy Leebov, Dr. Jan Gehler and others—who saw something in me and connected me to opportunities and experiences that were beyond my dreams as a young adult growing up in a small town in Northern New Mexico.
Chow, Rosalind, Don’t Just Mentor Women and People of Color. Sponsor Them. Harvard Business Review, June 2021.
The Platform and the Protégé
Kevin Monaco
When I first entered the workforce as a high school teacher at a small private school, I had very little knowledge of how to elevate my professional status, and I certainly did not know how to reach my audience. I had many mentors that eagerly shared their passion and knowledge for teaching and I enjoyed a great deal of collaboration with my colleagues. But as I gathered experience and honed my skills in the field, I began to feel that I could contribute at a higher level, in a greater capacity. There was one problem. I had little idea of how to get there. My deepening desire to expand my path led me to ask the questions: How can I surround myself with successful people whom I admire? How can I nurture a desire in them to invest in my success?
I began by identifying people in my life who could serve as my sponsors. Over time, I devoted purposeful attention to these relationships and they burgeoned into formal sponsor/protégé roles. When I reflect on the ways in which sponsorship has changed my career trajectory, the single most important part of the process has been the ‘platform.’ The platform is the protégé’s stage. It is their time to showcase their skills in front of a crucial audience. When we are given a platform, we can be directly involved in the process. Our role is amplified.
The sponsor shares this powerful tool as a way to leverage connections and bring the protégé into the fold. It provides purpose and focus for the protégé’s skills, imparting opportunities to get involved, demonstrate one’s capabilities, and create vital networks along the way. It enables others to notice the unique value the protégé adds within the field or institution. This is why the role of the audience is so critical to this process. When we are elevated on a platform, we can be recognized for our achievements. We can garner experiential growth opportunities that are vital to our professional advancement. We can strengthen our current skills and we can be supported in acquiring new ones.
But there is an important reciprocation as well. It is true that the sponsor carries the connections and social capital, but an effective sponsor/protégé relationship enriches the professional lives of both. This is why the relationship continues. While being teachable and receptive are important qualities of the protégé, it is important to note that the protégé must also be a willing contributor to the conversation, ready to step up to the plate! This is the essential charge of the protégé. It may seem like a lot of pressure, but we must understand an essential facet of the relationship. The foundational cornerstone of sponsorship is that of mutual respect. It is an indispensable ingredient for the success and continued forward movement of the relationship. There must be deep personal and professional respect between individuals in these roles, and respect leads to trust.
On a personal level, it is this precise trust in my sponsors that continues to provide me with the encouragement I need to level up. In a society that largely suffers from imposter syndrome (and I am no exception), we all need assurance at times that we have champions and cheerleaders in our corner. When we trust that we are respected and supported by experienced individuals in our fields, we feel capable of tackling the next stage. The expertise of the sponsor and the potential of the protégé collide to create a mosaic of collaboration, excellence, and purpose. It is through this amplification process that we expand our view of what is within our grasp.